What is Knee Osteotomy?
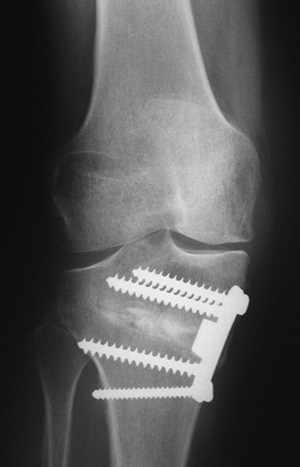
A tibial osteotomy is a procedure in which the upper part of the tibia (shin bone) is cut and wedged open in order to realign the leg. This in turn will release stress placed on the damaged cartilage and bone on the affected portion of the knee, thus redistributing the forces to more normal areas of the knee joint.
Your evaluation helps your surgeon determine if you are a candidate for a tibial osteotomy. During this time, these key areas will be addressed: medical history, physical exam and imaging (X-ray/MRI). Your medical history includes questions about knee pain, medications you may be taking, prior surgery, infections, bleeding disorders and other bone and joint problems you may have. Your physical examination includes assessing your range-of-motion (stiffness or instability), any deformity in your legs (bow-legged or knocked-kneed), and watching how you walk and sit. Finally, special x-rays of your knees will be obtained to show the degree of damage and deformity. This assessment will help determine if you are a candidate for an osteotomy and the amount of realignment correction needed.
A relatively small percentage of patients are candidates for these realignment procedures. Patients undergoing an osteotomy procedure for arthritis or degeneration are relatively young (e.g. below 50-55). Unlike a knee replacement, after a tibial osteotomy activity restrictions are minimal and the patient can return to high impact work and sports. After an osteotomy for arthritis, in appropriately selected patients, approximately 70-80% of patients will have good enough pain relief and function to avoid a knee replacement for greater than 10 years. They are also performed for certain types of knee instability and occasionally in cases of repeat ligament reconstruction to help protect the new ligament by realigning the leg.

Post Operative
A tibial osteotomy can lead to quite a bit of pain after surgery. This is normal. Narcotic medications are prescribed while in hospital and are continued at home. It is useful to combine the narcotic medications with acetaminophen.
Swelling and bruising are quite common after surgery. Some patients notice bruising up and down the limb. This needs to be watched closely, but it is generally normal. Icing can help with pain management and it can help control the bruising.
A cryocuff is a device that helps circulate ice water through a wrap around the knee. Many patients use this device to help manage pain and swelling after surgery. There is good research documenting the positive effect on pain relief of cryocuff treatment after surgery. Most extended health care plans will cover the majority of the cost.intelliflokneepad
You will wake up with a hinged brace on. You need to wear this at all time for the first 6 weeks after surgery. Further instructions are provided with your physiotherapy documents. Patients generally stay in hospital for 24-48 hours after surgery. tscopepremier_044
Physiotherapy: Physiotherapy should be started within one week after surgery. Physiotherapy is crucial as part of the management of an osteotomy and is not covered by the government.
Wound care: It is important you keep your wound dry until it is healed. The bulky dressing and tensor bandage can be removed before you leave hospital or at 2-3 days post-operatively. A clean protective dressing can they be reapplied. A dressing should be worn until the wound is completely dry.
Follow-up: After discharge, you will see your surgeon 10-14 days after surgery to remove stitches and answer any questions. The next follow-up with your surgeon is generally 6-8 weeks after surgery and an X-ray will be taken to assess healing. At this point you will likely be able to start putting weight on your leg and the brace will be discontinued.


Risks or Complications
These are relatively big operations that involve a short hospital stay. As with any surgical procedure, there are some risks involved. There is always a small risk associated with the use of general or spinal anesthesia. Antibiotics will be given during and after surgery to help decrease the risk of infection. You will be encouraged to get out of bed and become mobile soon after surgery to help decrease the risk of blood clots in your leg. In addition, this procedure carries a very small risk of injury to the nerves and vessels around the knee. There is also a small risk of the bone not healing, necessitating another surgery. This risk is minimized by avoiding anti-inflammatory pills and not smoking. In fact, smoking is absolutely not permitted in anyone considering this surgery. The patient must quit completely prior to surgery and avoid smoking entirely until the bone is healed.