What is Shoulder Instability?
Shoulder instability is the loosening of the ligaments and soft tissue surrounding the shoulder joint which allow the head of the humerus (ball) to shift in the glenoid (socket).
The shoulder is designed like a ball on a golf tee. There is a large ball sitting in a small cup. This design is very good to have a large range of motion but at the downfall of potential instability. In order to create more stability there are several soft tissue structures that surround the joint including the rotator cuff muscles (dynamic stabilizers), the labrum, ligaments and the shoulder capsule (static stabilizers).
Causes
Shoulder instability can be due to increase global ligament laxity or a traumatic event that leads to damage within the shoulder and recurrent dislocations. These two types of instability are treated differently.
Most commonly when there is a traumatic shoulder dislocation it is anterior or forward. The head of the humerus shifts forward and may get stuck on the front of the glenoid. When this occurs the labrum is torn along the front of the socket.
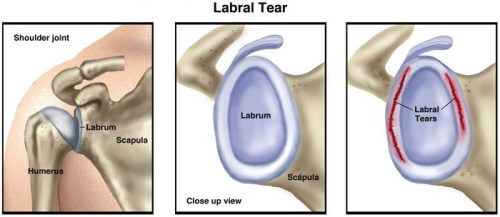
What is the labrum?
The labrum is a ring of soft tissue that surrounds the glenoid (socket). It acts to deepen the shoulder joint and is the attachment for important stabilizing ligaments and therefore increases the stability of the joint.
With a dislocation this labrum commonly tears (Bankart lesion) and allows the shoulder to dislocate more easily than previously. When it heals it often heals in an incorrect place and decreases its function. After a single dislocation, patients may have enough stable structures in the shoulder that they do not suffer from recurrent dislocations. After more than one dislocation, especially in young patients, the likelihood of further dislocations nears 100%. After each dislocation further damage is done to the labrum, ligaments and even the bone around the shoulder joint.
What are other injuries associated with shoulder dislocation?
Other injuries are possible with shoulder dislocation. Fractures of the front of the glenoid (socket) can occur and with frequent dislocations a gradual wearing away of the socket can occur making surgery more challenging and recurrent dislocations more common after surgery.
A Hill-Sachs lesion may also occur. This is an injury to the back of the humeral head (ball) that occurs when it dislocates and gets dented on the front of the glenoid (socket) like a ping pong ball. Commonly these are small and do not need to be addressed.
In patients over the age of 40, rotator cuff tears may occur with dislocation and this should be investigated with an ultrasound if the shoulder does not settle over 6-10 weeks after the dislocation.
What is the risk of recurrent shoulder dislocation?
The risk of dislocation is related inversely to age. When people dislocate for the first time in their teens their risk of recurrence is approximately 80%. This decreases with age, being much less common to have a repeat episode over the age of 40.
Treatment
After a single dislocation, most patients are managed non-operatively. This consists of wearing a sling for the first 3 weeks and then progressing to increase range of motion. Physiotherapy is very important to work on achieving increased stability. A focus is on the dynamic stabilizers of the shoulder, specifically the rotator cuff muscles and muscles around the scapula (shoulder blade).
This may be successful for maintaining stability and allowing for return to sporting activities. If you have recurrence after trying a dedicated physiotherapy program then surgical intervention will likely be suggested.
Arthroscopic Bankart Repair
In most patients with shoulder instability, arthroscopic labral repair is appropriate. Surgery is done arthroscopically, which means through “key hole” or small incisions. Typically, you will have 2 or 3 incisions that allow a camera and surgical instruments to be placed in the shoulder to assess the damage and complete the repair.
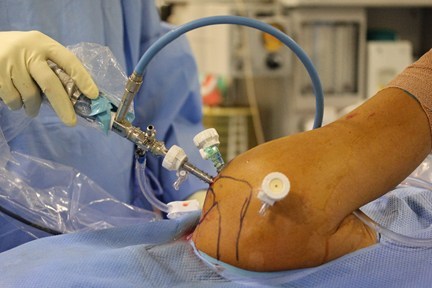
A camera and three cannulas are seen in this right shoulder with the patient lying on their left side.
The scarred labrum is elevated from the incorrect position and sutures are placed around it. The labrum is then secured back to its appropriate position on the edge of the glenoid (socket) using small anchors. This acts to re-tension the stabilizing ligaments, deepen the socket and create stability.
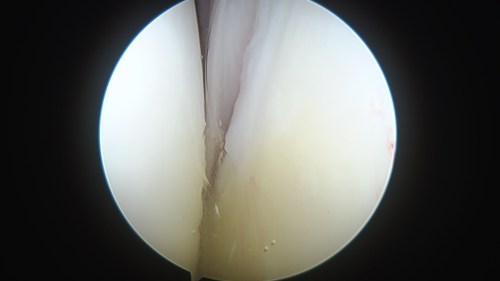
The humeral head is seen adjacent to the torn labrum.

Another view with the torn labrum in the middle of the page and the humeral head to the left.
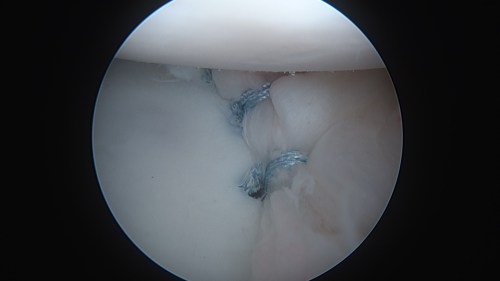
The labrum has been repaired to the glenoid using 3 stitches and anchors.
In some patients with a high number of dislocations and wear of the socket or in patients who have failed a previous surgery, an open procedure with bone grafting may need to be performed. This procedure is called a Latarjet procedure and involves the transfer of a small bone (coracoid) to the glenoid (socket) in order to make the socket larger.
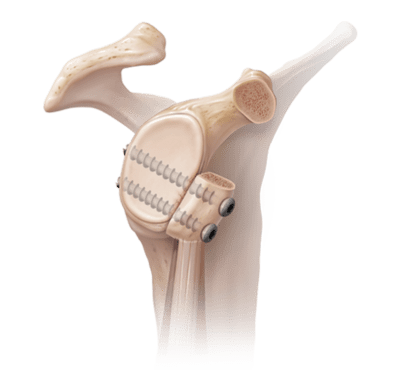
A latarjet procedure: the coracoid bone is grafted to the front of the glenoid to ‘extend’ the socket.
After shoulder surgery for instability the expectations and requirements are similar regardless of the procedure and can be found on the shoulder arthroscopy page.