What is a Meniscus Tear?
The menisci are fibrocartilaginous structures in the knee joint that sit between the tibia and femur. There is one on the medial (towards the middle) and one on the lateral (towards the outside) sides of the knee. The ends of the bones have articular cartilage on their surfaces which is a shiny, white, low friction tissue that is the bearing surface of the joint (the white tissue at the end of a chicken bone).
The end of the femur is round and the top of the tibia is flat. The menisci help to improve the congruity between the two bones to decrease the force across the smooth cartilage.
The menisci have several functions and the most important may be shock absorption but they also have secondary roles as joint stabilizers, as well as lubrication and nutrition for the cartilage.
Meniscus tears are very common. Loss of function of the meniscus as a result of a tear can lead to a feeling of catching pain or locking as the loose flap gets caught with motion of the knee. Without the shock absorption function of the meniscus increased pressure is felt by the cartilage across the joint resulting in early wear and tear. However, approximately 20% of people without any symptoms are found to have meniscus tears on MRI examinations.
Causes
Meniscal tears can occur as a result of trauma such as a twisting force but they are also part of the spectrum of pathology seen in the development of knee osteoarthritis.
Diagnosis
Diagnosis of meniscal tears starts with a history and physical examination by your family physician or a specialist. X-rays are always required when a patient is assessed for a potential meniscal tear to look for other causes for the symptoms for example arthritis. If suspicion is high for a meniscal tear and the patient is a good candidate for surgery then moving to knee arthroscopy may be suggested. If there is doubt about the presence of a meniscal tear then an MRI can be ordered to assess the soft tissue structures of the knee which include the menisci.
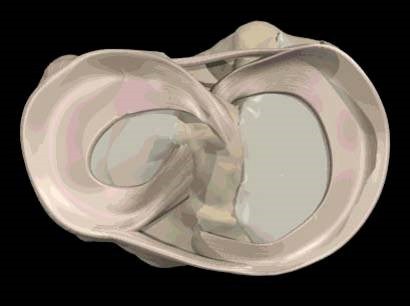
Figure 1: The lateral and medial menisci attach near the centre of the tibia.
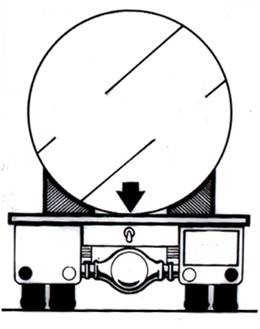
Figure 2: The menisci act like these chocks to stabilize and support the round load (Femur) on a flat surface (Tibia)
Surgical Treatments
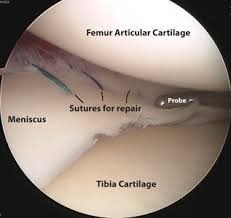
Treatment of meniscal tears depends a great deal on the age of the patient. In young patients, for example under the age of 35 or 40 meniscal tears are most commonly as a result of a trauma. In these cases, knee arthroscopy can be performed to assess the meniscus and treat it accordingly. If possible, meniscus tears should be repaired with stitches especially in young patients in order to preserve their function.
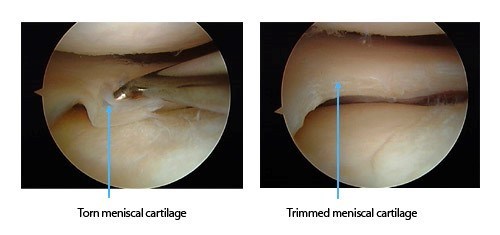
In most cases, even in young patients, meniscal tears are not amenable to repair and must be resected. A ‘partial meniscectomy’ is the removal of the unstable portion of the torn meniscus. The goal is to leave the patient with as much healthy meniscal tissue as possible in order to preserve as much of the function as possible.
In older patients, for example those older than 45 or 50 years, the cause of the meniscus tear and treatment protocols are usually very different. We now know that degenerative meniscal tears are very common in people as they get older. They are thought to be most commonly the result of age related degenerative change in the knee not acute trauma. Therefore, the symptoms, especially achy discomfort are most likely related to early wear and tear NOT the meniscal tear.
Much research has been conducted on degenerative meniscal tears in the last 5-10 years. There are a number of excellent research studies (double blind randomized placebo controlled trials) which have demonstrated that patients with degenerative meniscal tears respond equally well to non-operative management when compared to arthroscopic surgery. This includes patients without any signs of arthritis on their X-rays. Therefore, first line treatment for patients with degenerative meniscus tears should be a thorough non-operative program.
Patients with signs of significant arthritis on X-rays should not undergo MRI examination to look for meniscal tears for two reasons. Firstly, there will almost certainly be a meniscus tear found on the MRI because they occur in association with knee arthritis and the meniscus tear is not the cause of the pain, the arthritis is. Second, numerous studies have been performed dating back to the mid-nineties that have left no doubt that knee arthroscopy for debridement or partial meniscectomy in the presence of significant knee arthritis does not work.
Patients with degenerative meniscal tears can respond very well to appropriate non-operative care and this care should be initiated by their family physician.