What is Femoroacetabular Impingement?
Femoroacetabular impingement or FAI simply describes the action of the femoral neck hitting the edge of the hip socket. In cam type impingement the edge of the ‘ball’ of the hip has a bump on it making the ball more of an oval. When the hip is moved through a range of motion the oval ball must try to rotate into a round socket which results in abnormal contact between the structures as a result of the mismatch in shape. In the case of pincer impingement, a round ball is present but the socket is too deep or has a prominent edge causing the femoral neck to contact the edge of the socket with motion of the hip.
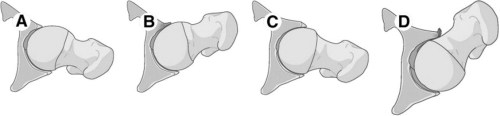
A and B: The cam lesion comes forward and hits the labrum C and D: The normal femoral neck comes forward and strikes the “pincer”
There is a wide range of normal anatomy. Some people have a narrow femoral neck and thus their hip has to move a long way before it will impinge. Others have a much thicker femoral neck and they do not have to flex their hip very far before it will impinge. This thick bony bump at the junction of the femoral head and the femoral neck at the front is known as a cam lesion. In the case of a pincer lesion, it simply denotes a hip socket that is very deep or an isolated prominent rim at the front or back of the socket. In a normal pelvis the hip sockets face forward but in some patients, they face sideways or even slightly backwards (retroverted acetabulum). In these patients, the front rim of the socket is prominent and impinges relatively easily.

The cam lesion is seen at the junction of the femoral head and neck.
What gets damaged by the impingement?
When a patient with a cam lesion flexes up their hip too far, the bony bump must be accommodated within the rigid hip socket. This is like trying to get an egg into an egg cup, sideways. It just won’t work. The bump strikes the labrum and then starts to shear the articular cartilage (gliding surface of the hip) causing it to peel away from the underlying bone. The flap of damaged cartilage can become painful and the area of damaged cartilage can become larger and larger with time. This eventually leads to osteoarthritis and for a number of patients, a hip replacement. During this process the labrum is also damaged and may be seen on the MRI.
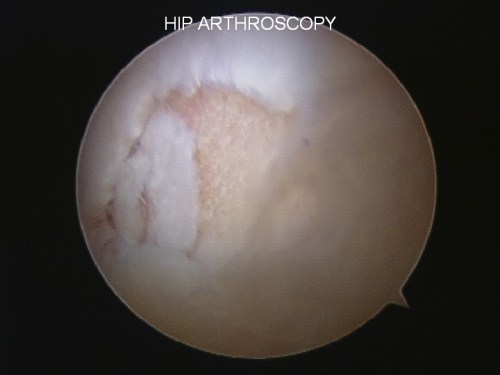
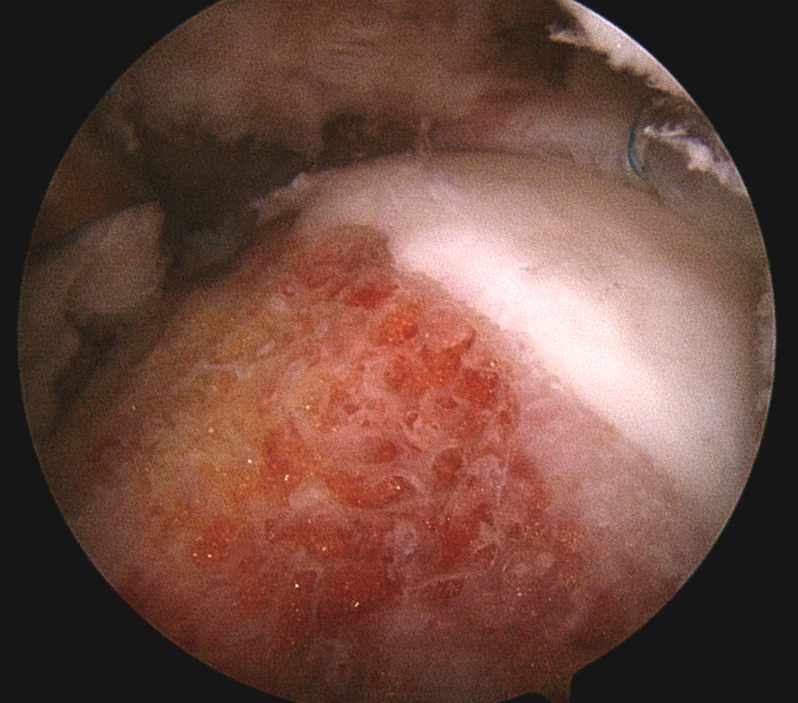
The cam lesion has damaged the white gliding surface (articular cartilage) The yellow is the underlying bone.
With a pincer type of impingement (a deep cup or a prominent hip socket rim) the labrum is the first structure to be damaged. When the femoral neck forcibly hits the labrum, it is torn from the edge of the socket and becomes painful. This type of impingement too can lead to osteoarthritis.
At what age does FAI present?
Labral and cartilage tears can and do occur in the adolescent athlete. The most common age for a patient with cam type impingement to present would be a 20-30 year old man. Being active in kicking sports and sports such a hockey where the athlete pushes against a flexed hip are common findings. The most common age for the pincer type impingement to present would be a woman in her 30’s or early 40’s.
When is it too late?
Every patient and situation is different. It is common for middle aged and older adults to present with groin pain. Unfortunately, in this patient population usually the groin pain is due to early arthritic pain that will not respond well to hip arthroscopy. If an MRI is performed in someone with arthritis it will show a labral tear virtually every time. The labral tear is not the problem. The arthritis is the problem.
If the joint space of the hip on a weight-bearing X-ray has narrowed, it usually means the arthritic process is too advanced and the patient will not benefit from arthroscopic treatment. X-rays are always necessary in the work up of patients with hip pain. They should always be performed before an MRI because they may show arthritis and mean the expensive MRI is totally unhelpful.
If a patient has enough arthritic change to preclude hip arthroscopy then a change in lifestyle will be suggested including: non impact exercise such as cycling, weight loss (where appropriate), anti-inflammatory medication and if needed injections into the joint (e.g. Hyaluronic acid, Platelet rich plasma or cortisone). When non-operative management has stopped working a hip replacement may be considered.

This young male athlete still has a good joint space on the left hip (right side of picture) but unfortunately the right hip is well past the stage when arthroscopic surgery would be helpful.
Surgical Treatments
If a period of rest followed by rehabilitation and alteration of aggravating activities does not result in improvement in symptoms then surgery can be considered. Arthroscopic surgery is performed as a daycare procedure. This is done by reshaping the abnormal bony anatomy to a more normal shape using the arthroscopic instruments.
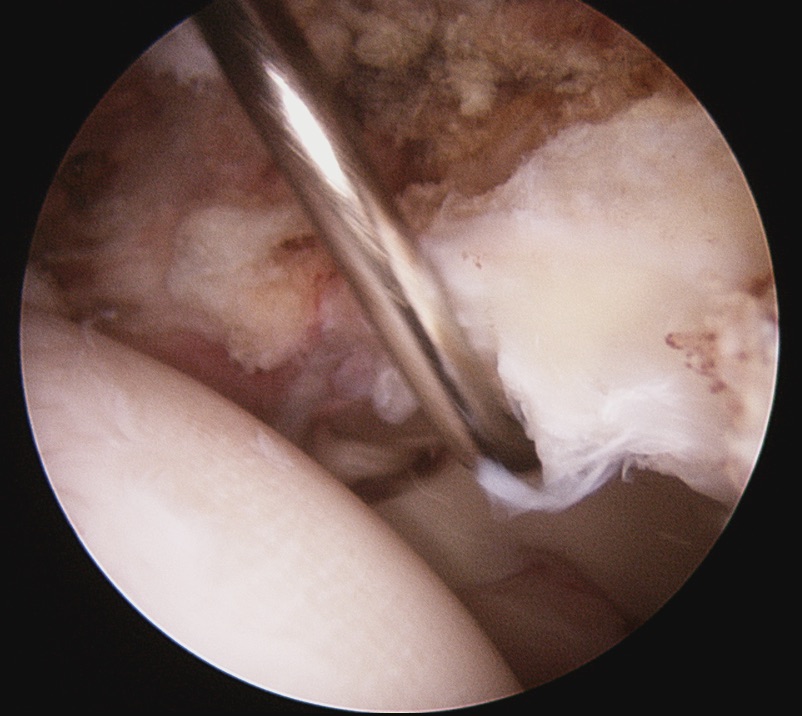
A probe is hooked under a labral tear.
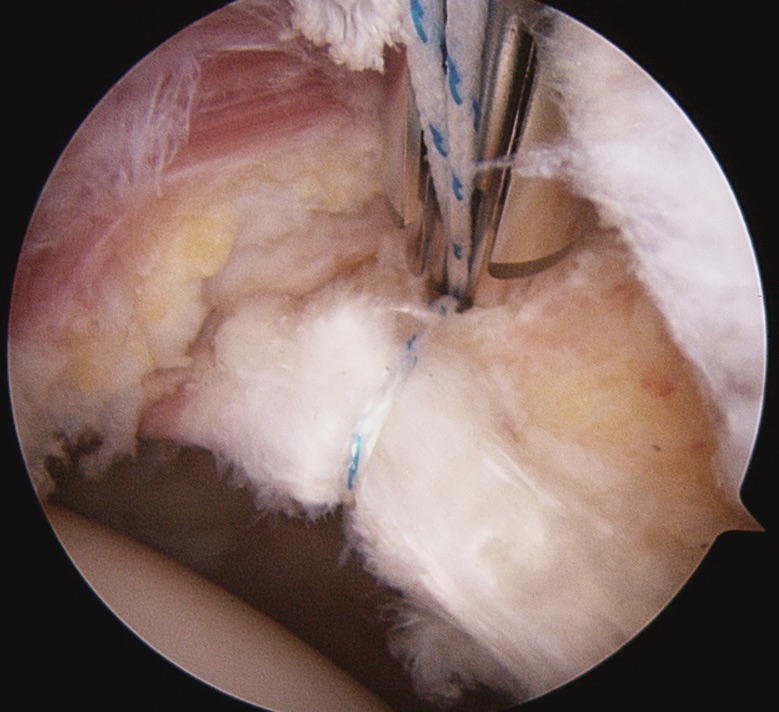
A suture is around the labrum and an anchor is being placed into the bone above the hip socket.

The labrum has been repaired with 3 anchors. 2 of them are visible in this picture.
The red and yellow is the raw bone of the femoral neck after the cam lesion was removed with a bur. One of the labral sutures can be seen at 1 o’clock.